TECHNIQUE
The ultrasonography of the elbow joint is performed with the patient seated in front of the examiner with the elbow placed on an examination table or with the patient in the supine position.
It is important to perform a dynamic evaluation with varying degrees of patient arm rotation and joint stress manoeuvres and,
owing to the curvilinear contours of this articulation,
a careful scanning technique is critical.
A high frequency linear transducer (12-17 MHz) should be used.
The evaluation of the elbow can be divided into four compartments that will be described in detail: anterior,
lateral,
medial and posterior.
ANTERIOR ELBOW
For the initial evaluation of the anterior elbow,
the arm is extended and the forearm is in an extended and supinated position,
sometimes supported by placing a pillow under the joint.
The examination should include both transverse and longitudinal planes extending at least 5 cm proximal and 5 cm distal to the joint.(Fig. 1)

Fig. 1: Anterior elbow approach
The key structures to be evaluated anteriorly include:
1- Anterior joint recess
2- Distal brachialis muscle
3- Distal biceps brachii muscle
4- Median nerve
With the probe positioned at the level of the brachialis muscle both in transverse and medial sagittal plan,
the anterior coronoid recess and smaller radial fossa of elbow joint are visualized.
These normally appear as concavities of the anterior surface of the distal humerus,
filled with the anterior fat pad.
(Fig. 2) A small amount of normal fluid may be seen between the anterior fat pad and humerus.
The anterior distal humeral epiphysis is best scanned in the longitudinal plane to visualize the capitellum and radiocapitellar joint laterally and humeral trochlea and ulnotrochlear joint medially.
The articular surfaces appear as a wavy hyperechoic line covered by a thin layer of hypoechoic articular hyaline cartilage,
which is covered by a thin hyperechoic line representing the anterior joint capsule (2 mm in average in the adult population).
(Fig. 3)
- Distal brachialis muscle/tendon
The brachialis muscle,
which essentially acts as a flexor of the elbow,
is best evaluated with the transducer in the longitudinal plane over the anterior supracondylar region of the distal arm.
The brachialis muscle lies deep to the biceps brachii and anterior to the humerus.
It demonstrates hypoechoic muscle fascicles with intervening hyperechoic fibroadipose septa,
findings characteristic of muscle tissue.
(Fig. 2 and Fig. 3)
To evaluate the brachialis tendon and its insertion on the proximal ulna (coronoid process) with US,
transverse and longitudinal planes are useful.
- Distal biceps muscle/tendon
Distal biceps tendon (DBT) is a flexor of the elbow but also a supinator,
which is best evaluated with the patient’s forearm in maximal supination to bring the tendon insertion at the radial tuberosity into view.
Because identification of the DBT can be difficult,
it is often helpful to begin evaluation in the transverse plane.
With movement of the probe from proximal to distal,
one can identify the biceps brachii muscle superficial to brachialis muscle and lateral to median nerve and brachial artery,
which is easily seen and because of that it can be used as a landmark. (Fig. 5) Once the DTB is identified the transducer is turned 90º to evaluate the tendon longitudinally.
(Fig. 4)
Because the DBT courses deep away from the transducer in a oblique fashion,
this segment of the tendon appears artifactually hypoechoic from anisotropy.
This can be reduced with application of more pressure on the transducer distally to obtain a more perpendicular relationship between the sound beam and the tendon fibers or an evaluation with various degrees of elbow flexion and extension may also help.
In most individuals,
The DBT is formed by union of two muscle bellies: the short and long heads of the biceps brachii.
The tendon of the long head of the biceps inserts proximally while the tendon of the short head of the biceps inserts distally.
Persistent division of the short and long heads of the DBT is an important anatomic variant to be aware of to avoid incorrect diagnosis as a DBT partial tear.
At the elbow,
the median nerve is medial to the brachial artery and can be followed distally as it courses between the humeral and ulnar heads of the pronator teres,
in most individuals.
In cross section it has a honeycomb appearance because of hypoechoic nerve fascicles and hyperechoic connective tissue.
(Fig. 5)
LATERAL ELBOW
For evaluation of the lateral elbow structures,
in general the elbow is in extension,
thumb up,
or with the elbow in flexion and the forearm in internal rotation.
(Fig. 6)
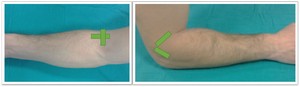
Fig. 6: Lateral elbow approach
The key structures to be evaluated in the lateral elbow include:
1- Radiocapitellar joint and capitellum
2- Common extensor tendon
3- Lateral collateral ligamentous complex
4- Annular recess
5- Radial nerve
- Radiocapitellar joint and Capitellum
To begin the evaluation,
the probe must be placed in the longitudinal plane to scan the articulation of the radial head with the capitellum,
which appears a hyperechoic contour,
easily identifiable.
(Fig. 2 and Fig. 10)
The common extensor tendon is the primary extensor of the wrist and hand,
which consist of the tendon of four contributing muscles: the extensor carpi radialis brevis,
extensor digitorum communis,
extensor digiti minimi and extensor carpi ulnaris.
Longitudinal planes are the best to visualize the beak-shaped hyperechoic origin of the common extensor tendon between the subcutaneous tissue and the radial collateral ligament. (Fig. 8) The single contributions from the extensor muscles to the common extensor tendon cannot be identified at US.
Transverse planes should also be obtained over the tendon insertion,
which appears oval shape,
superficially to the bone of the lateral epicondyle.
- Lateral collateral ligamentous complex
The lateral collateral ligamentous complex provides stability to the lateral elbow joint.
It is composed of several components: the radial collateral ligament (RCL),
the lateral ulnar collateral ligament (LUCL) (Fig. 9),
part of the annular ligament (AL) (Fig. 10),
and sometimes an accessory radial collateral ligament.
The RCL is a thick band of hyperechoic fibers,
which arises from the anteroinferior lateral epicondyle and converges with the fibers of the annular ligament distally on the radius.
The LUCL is the major stabilizer against varus stress and posterolateral rotatory instability.
This distinct and tightly fibrillated structure originates at the posteroinferior lateral epicondyle deep to the common extensor tendon and posterior to the RCL origin.
It is best evaluated with the transducer placed over the proximal RCL and angled posteriorly toward the ulna. (Fig. 9 and Fig. 10)
At the level of the radial neck,
the collapsed annular recess is difficult to discern,
unless it is abnormally distended by fluid.
This evaluation can be helped with dynamic imaging during passive pronation and supination of the forearm.
The radial nerve has a hypoechoic appearance in cross section.
Proximally,
it may be identified over the posterior aspect of the humeral diaphysis,
where it moves medially to laterally behind the humeral shaft within the radial groove.
Then it is followed distally as it travels deep to the brachioradialis and brachialis muscles.
(Fig. 11)
At the level of the elbow joint,
the radial nerve bifurcates into the superficial cutaneous sensory branch and the posterior interosseous nerve. (Fig. 11) To evaluate these very small nerves,
dynamic transverse US images are used,
because it is difficult to recognize small monofascicular nerves on static US images.
MEDIAL ELBOW
For evaluation of the medial elbow structures the patient’s forearm is placed in forceful external rotation while keeping the elbow extended or slightly flexed,
resting on a table.
(Fig. 12)

Fig. 12: Medial elbow approach
The key structures to be evaluated in the medial elbow include:
1- Medial epicondyle
2- Common flexor tendon
3- Anterior band of the ulnar collateral ligament (UCL)
Sonographic evaluation of the medial elbow structures begins by visually identifying or palpating the medial epicondyle of the humerus.
The transducer is then placed in the longitudinal plane to the forearm with the proximal aspect over the medial epicondyle.
The characteristic hyperechoic bony contours of the medial epicondyle and ulnotrochlear articulation will be seen. In this plane,
both the common flexor tendon and the anterior band of the UCL can be identified.
(Fig. 13 and Fig. 14)
The common flexor tendon supports the ulnar collateral ligament in resisting valgus stress and is the primary flexor of the wrist and hand.
It consists of the tendon of four contributing muscles: flexor carpi radialis,
palmaris longus,
flexor carpi ulnaris,
and flexor digitorum superficialis.
The origin of the common flexor tendon should be seen at the most medial aspect of the medial epicondyle as hyperechoic and fibrillary pattern,
with transition to hypoechoic musculature more distally.
(Fig. 13) This tendon appears larger but shorter than the common extensor tendon.
The UCL is the chief stabilizer of the elbow against valgus stress when it is flexed more than 20°.
This ligament complex is composed of the anterior,
posterior and transverse band.
The anterior band is functionally the most important,
since it provides the greatest degree of stabilization.
It originates from the anteroinferior aspect of the medial epicondyle,
extends distally over the joint space to insert on the sublime tubercle of the coronoid process of the ulna.
(Fig. 14) More adequate positioning for examination of this ligament is obtained with the patient supine keeping the shoulder abducted and externally rotated and the elbow in 90° of flexion.
In US normally appears as hyperechoic,
thin and compact fibrillar band just deep to the common flexor tendon.
(Fig. 14) As with all ligaments,
the anterior band of the UCL can appear artifactually hypoechoic from anisotropy.
The posterior band inserts distally at the posteromedial margin of the trochlear notch of the ulna and acts against internal rotation.
The transverse band does not cross the elbow joint; therefore,
it may not have a relevant stabilizing function.
POSTERIOR ELBOW
For evaluation of the posterior elbow structures the patient should flex the elbow at 90° with the forearm fully pronated (internally rotated),
and the palm resting on a table.
If the patient is supine,
he should place his hand across the abdomen,
with the arm abducted,
flexed,
and internally rotated.
(Fig. 15)
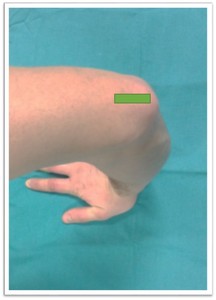
Fig. 15: Posterior elbow approach
The key structures to be evaluated in the posterior elbow include:
1- Posterior joint recess
2- Olecranon bursa
3- Distal triceps muscle and tendon
4- Ulnar nerve and cubital tunnel
To start the evaluation of the posterior structures,
the probe can be place posteriorly in the sagittal plane,
over the proximal elbow,
where the characteristic hyperechoic shadowing bone contour of the humerus is identified.
As the humeral diaphysis approaches the elbow joint,
there is a pronounced concavity,
which represents the olecranon fossa.
(Fig. 16) This fossa is normally filled with the hyperechoic posterior elbow fad pad,
and it is the preferred site for evaluation of joint fluid and intra-articular bodies.
With the elbow in extension,
the olecranon bursa superficial to the olecranon process and distal triceps tendon,
can be evaluated.
In evaluation for olecranon bursal fluid it is important to use a thick layer of gel and minimal transducer pressure,
because this will ensure that bursal fluid is not displaced out of the field of view.
- Distal triceps muscle and tendon
The triceps muscle consists of three heads,
medial,
lateral and long.
The lateral and the long heads converge distally to form a common tendon that inserts posterior to the insertion of the medial head on the proximal portion of the olecranon process of the ulna (approximately 1 cm distal to the tip of the olecranon).
The predominantly hypoechoic triceps muscle and the hyperechoic distal triceps tendon are seen superficial to the olecranon recess and should be evaluated in both transversal and longitudinal planes.
(Fig. 16)
- Ulnar nerve and cubital tunnel
The ulnar nerve supplies the flexor carpi ulnaris and the medial half of the flexor digitorum profundus muscle at the level of the elbow.
At the level of the elbow,
proximally the ulnar nerve is located in the cubital tunnel,
a fibro-osseous channel formed by the olecranon process laterally,
medial epicondyle medially,
posterior bundle of the UCL and joint capsule anteriorly,
and cubital tunnel retinaculum (Osborne ligament) posteriorly.
Distally it lies deep to the arcuate ligament,
an aponeurotic attachment of the two heads of the flexor carpi ulnaris muscle.
For the evaluation of the cubital tunnel,
the elbow may be fully extended and the arm internally rotated to avoid compression of the ulnar nerve at the cubital tunnel.
A 10–15 MHz probe and a large amount of gel,
should be preferably used.
The transducer is placed in a transverse plane between the hyperechoic bony protuberances of the olecranon process and medial epicondyle.
In this transverse approach the ulnar nerve is seen as an oval structure that,
sometimes appears with a hypoechoic fascicular pattern.
(Fig. 17 and Fig. 18)


















